- Credits
- Section Writer: Dr. Om J Lakhani
- Section Editor: Dr. Om J Lakhani
- Video lecture : Dr. Alpesh Goyal
- Q. What are the causes of hypothyroidism in cancer patients ?
- • Drug induced
- - Conventional anticancer agents
- Targeted cancer therapy
- Cancer immunotherapy
- • Radiation to CNS or thyroid
- • lodinated contrast use.
- Q. True or false- those patients who develop hypothyroidism due to anti-cancer use are more likely to have better response to cancer treatment ?
- Some studies have suggested this to be true
- However this is controversial
- Could be an elemental of bias
- However may be potentially true for immunotherapy
- Q. What are the various types of conventional anti-cancer drugs ?
- Alkylating agents : Cisplatin, Carboplatin, Cyclophosphamide, Temozolomide
- Antimetabolites: Methotrexate, Capecitabine, Azacitadine, 5-Flurouracil
- Anthracyclines: Doxorubicin, Daunorubicin
- Topoisomerase inhibitors: Irinotecan, Topotecan, Etoposide
- Mitosis inhibitors: Paclitaxel, Docetaxel, Vincristine, Vinblastine
- Miscellaneous: Asparaginase, Arsenic trioxide, ATRA, Mitotane
- Q. Which of these drugs increase TBG levels ?
- Mitotane
- 5-FU
- Asparginase
- Q. What other type of thyroid dysfunction do you see with [[mitotane]] ?
- Mitotane can produce [[Central hypothyroidism]]
- Q. Which are the various forms of Targeted anti-cancer drugs ?
- Tyrosine kinase inhibitors: Imatinib, Dasatinib, Nilotinib, Sunitinib, Sorafenib, Motesanib
- Monocional antibodies: Bevacizumab, Rituximab, Panitumumab, Alemtuzumab
- Proteasome inhibitors: Bortezomib, Carfilzomib
- RXR agonist: Bexarotene
- lodine based cancer therapy : 1131 MIBG therapy
- Immunotoxins: Denileukin Difitox
- mTOR inhibitors: Temsirolimus, Sirolimus
- PARP inhibitors: Olaparib
- CDK inhibitors: Ribeciclik, Dalhocielih
- Q. Which of these produce hypothyroidism ?
- All the tyrosine kinase inhibitors
- Alemtuzumab
- Bexerotene
- I-131 MIBG
- Q. Which are hormone based cancer therapies ?
- Anti-androgens: Abiraterone, Bicalutamide, Cyproterone, Flutamide
- Anti-estrogens and Als: Exemestane, Fulvestrant, Tamoxifen, Letrozole, Anastrozole
- GnRH analogues: Goserelin, Histrelin, Leuprolide, Triptorelin
- Peptide Hormones: Lanreotide, Octreotide, Pasireotide
- Q. What is the impact of Tamoxifen on thyroid function ?
- Tamoxifen would increase the TBG levels
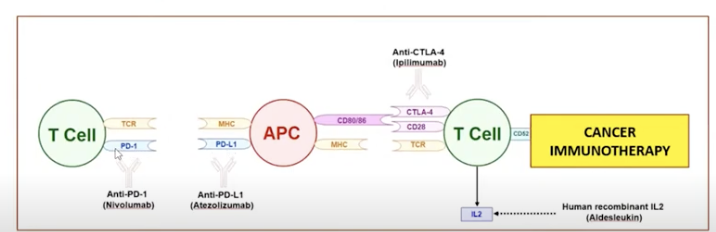
- Q. Which are the various immune check point inhibitors ?
- Antibodies against CTL4
- Ipilimumab
- Tremelimumab
- Antibodies against PD-1
- **Pembrolizumab** (**Keytruda**) ·
- Nivolumab (**Opdivo**) ·
- Cemiplimab (Libtayo)
- Antibodies against PD-L1
- **durvalumab**
- atezolizumab
- avelumab
- Q. How do tyrosine kinase inhibitors produce thyroid dysfunction ?
- By two methods
- 1. Increasing the requirement of levothyroxine in patients who are athyreotic
- This is especially true with Imatinib and the dose of LT4 must be doubled in such patients when initiated on imatinib
- Typically almost always occurs within 2 weeks of starting the drug
- The enhanced thyroid hormone metabolism attributed to increased Type 3 deiodination.
- 2. New onset of thyroid dysfunction
- This is seen with Sunitinib and Sorafenib
- TKI → inhibits VEGF → ischemic thyroiditis → thyroid dysfunction
- This effect is often delayed and occurs about 4-94 weeks after starting the drug
- Q. Bexrotene is used in what patients ?
- It is mainly used in patients with Cutaneous T cell lymphoma
- It is a RXR agonist
- Q. What type of hypothyroidism is seen with Bexarotene ?
- Mainly central hypothyroidism
- It is very rapid and occurs within hours
- It reduces TSH-beta gene transcription
- It can also suppress thyrotropes
- Q. What is Alemtuzumab ?
- Classification: Alemtuzumab is a humanized monoclonal antibody.
- Target: It is directed against CD52, a protein present on the surface of mature lymphocytes, but not on the stem cells from which these lymphocytes are derived.
- Usage in Therapy:
- It is used in the treatment of chronic lymphocytic leukemia (CLL) and multiple sclerosis (MS).
- In CLL, it is used for B-cell chronic lymphocytic leukemia, particularly for patients who have been treated with alkylating agents and have failed fludarabine therapy.
- In MS, it's administered to reduce relapses in relapsing-remitting multiple sclerosis.
- Mechanism of Action:
- Induces lysis of lymphocytes through antibody-dependent cell-mediated cytotoxicity and complement fixation.
- Leads to profound lymphopenia, thus modulating the immune responses.
- Administration: It is typically administered intravenously.
- Q. What kind of thyroid dyfunction is produced by Alemtuzumab?
- It produces [[Graves' disease]]
- This is mainly because of IRIS or immune reconstitution
- It is mainly seen in Multiple sclerosis patients given this drug
- Typically occurs after 6-31 months after giving the therapy
- Q. How is iodine given before MIBG scan ?
- Lugol's iodine, 5-6 drops, 3-5 times/day, beginning 1 d before and till 6 d after therapeutic/diagnostic MIBG
- Q. What type of autoimmune diseases are seen with Cancer immunotherapy or [[Immune checkpoint inhibitors]] therapy ?
- Mainly those induced by T-cells
- It mainly leads to T-cell activation and destruction of Cancer cells
- 
- Q. What are the various thyroid disorders seen with [[Immune checkpoint inhibitors]] ?
- Central hypothyroidism due to [[hypophysitis]]
- Primary hypothyroidism
- Painless thyroiditis
- Transient thyrotoxicosis
- Graves disease
- Euthyroid orbitopathy
- Q. Of the various immune check point inhibitors, what are the differential actions on various endocrine organs ?
- [[CTLA-4 inhibitor]] - [[Ipilimumab]]
- more involvement of Pituitary^^
- Pituitary gland expresses. CTLA-4 - hence more pituitary involvement
- Generaly occurs about 9 weeks after initiation of therapy
- [[PD1 inhibitor]] - [[Nivolomumab]] or [[Pembrolizumab]]
- more involvement of Adrenal and Thyroid #ClinicalPearl
- It can also cause [[Type 1 Diabetes]]
- Both type 1 and hypophysitits can coexist in the same patient
- Q. How common is central hypothyroidism with [[Ipilimumab]] ?
- Almost 100%
- This drug is common in metastatic melanoma
- Pituitary enlargement is almost commonly seen which resolves on discontinuation of the drug
- Q. What kind of thyroid dysfunction is seen with [[interferon alpha]] ?
- Autoimmune thyroiditis- mainly hypothyroidism- rarely even Graves' disease
- Q. Summarize the thyroid dysfunction seen with various anti-cancer drugs
- 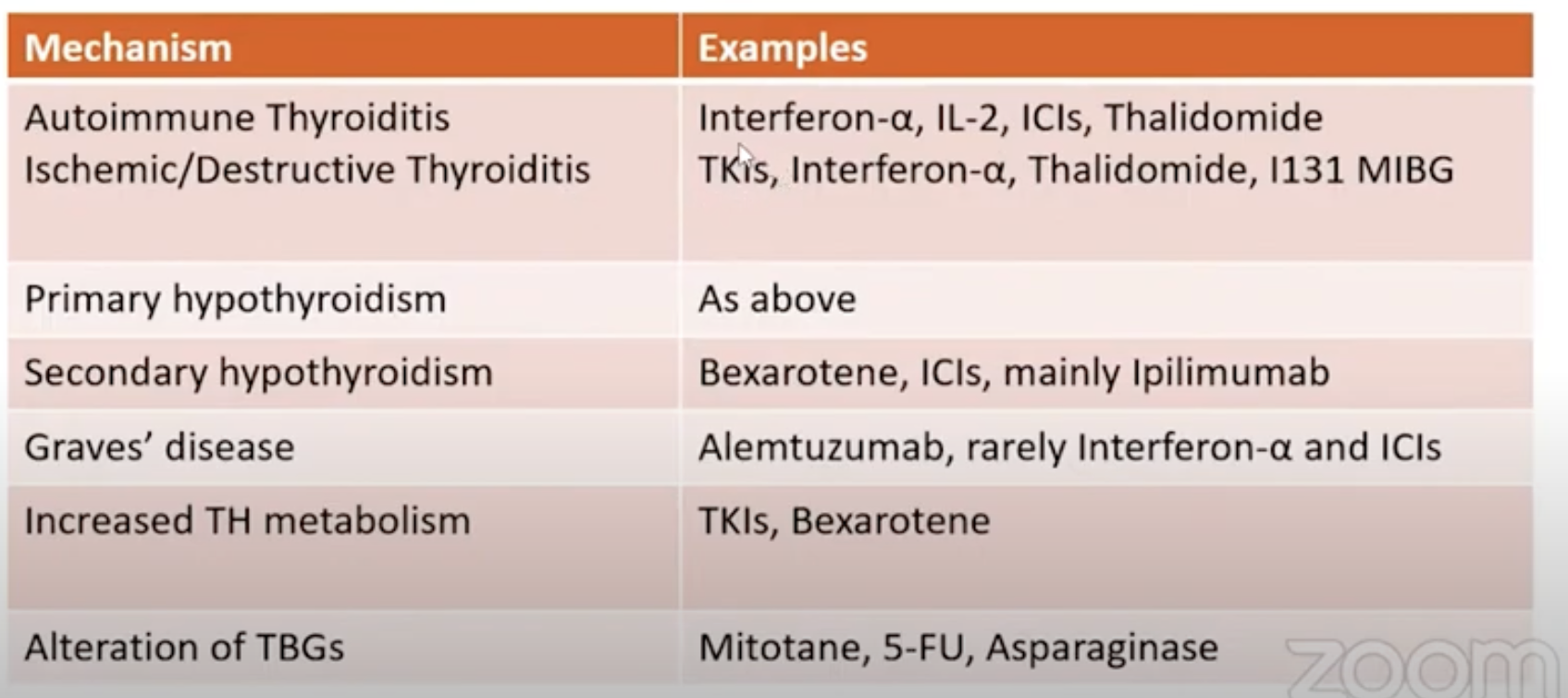
- Q. How should you monitor patients on [[Immune checkpoint inhibitors]] ?
- TSH, free T4, 8 am cortisol before x and before each cycle
- Consider baseline MRI pituitary
- Keep a close watch for mass effects, hyponatremia
- Low threshold for hormonal evaluation and MR imaging
Video lecture- by Dr. Alpesh Goyal
<iframe width="560" height="315" src="https://www.youtube.com/embed/hGP_EGwhHDw" title="YouTube video player" frameborder="0" allow="accelerometer; autoplay; clipboard-write; encrypted-media; gyroscope; picture-in-picture; web-share" allowfullscreen></iframe>
Reference:
1. Bhattacharya S, Goyal A, Kaur P, Singh R, Kalra S. Anticancer drug-induced thyroid dysfunction. European Endocrinology. 2020 Apr;16(1):32.